Paul Krugman and Robin wells, writing in the New York Review of Books.
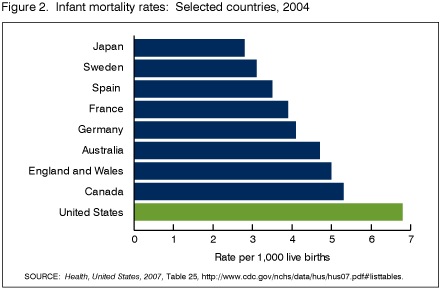
This inefficiency is a bad thing in itself. What makes it literally fatal to thousands of Americans each year is that the inefficiency of our health care system exacerbates a second problem: our health care system often makes irrational choices, and rising costs exacerbate those irrationalities. Specifically, American health care tends to divide the population into insiders and outsiders. Insiders, who have good insurance, receive everything modern medicine can provide, no matter how expensive. Outsiders, who have poor insurance or none at all, receive very little. To take just one example, one study found that among Americans diagnosed with colorectal cancer, those without insurance were 70 percent more likely than those with insurance to die over the next three years.
In response to new medical technology, the system spends even more on insiders. But it compensates for higher spending on insiders, in part, by consigning more people to outsider status—robbing Peter of basic care in order to pay for Paul’s state-of-the-art treatment. Thus we have the cruel paradox that medical progress is bad for many Americans’ health.
The idiosyncratically American practice of tying health care to employment is heading for a crisis.
Providing health insurance looked like a good way for employers to reward their employees when it was a small part of the pay package. Today, however, the annual cost of coverage for a family of four is estimated by the Kaiser Family Foundation at more than $10,000. One way to look at it is to say that that’s roughly what a worker earning minimum wage and working full time earns in a year. It’s more than half the annual earnings of the average Wal-Mart employee.
Health care costs at current levels override the incentives that have historically supported employer-based health insurance. Now that health costs loom so large, companies that provide generous benefits are in effect paying some of their workers much more than the going wage—or, more to the point, more than competitors pay similar workers. Inevitably, this creates pressure to reduce or eliminate health benefits. And companies that can’t cut benefits enough to stay competitive—such as GM—find their very existence at risk.
Once consequence of this trend is that Medicaid is under increasing pressure.
Medicaid has grown rapidly in recent years because i has been picking up the slack from the unraveling syste of employer-based insurance. Between 2000 and 2004 th number of Americans covered by Medicaid rose by remarkable eight million. Over the same period the ranks o the uninsured rose by six million. So without the growth o Medicaid, the uninsured population would have exploded and we’d be facing a severe crisis in medical care
But Medicaid, even as it becomes increasingly essential to tens of millions of Americans, is also becoming increasingly vulnerable to political attack. To some extent this reflects the political weakness of any means-tested program serving the poor and near poor. As the British welfare scholar Richard Titmuss said, “Programs for the poor are poor programs.” Unlike Medicare’s clients—the feared senior group—Medicaid recipients aren’t a potent political constituency: they are, on average, poor and poorly educated, with low voter participation. As a result, funding for Medicaid depends on politicians’ sense of decency, always a fragile foundation for policy.
The Bush administration’s response to the problem is to push consumer-directed health care. Bad idea.
What’s wrong with consumer-directed health care? One immediate disadvantage is that health savings accounts, whatever their ostensible goals, are yet another tax break for the wealthy, who have already been showered with tax breaks under Bush. The right to pay medical expenses with pre-tax income is worth a lot to high-income individuals who face a marginal income tax rate of 35 percent, but little or nothing to lower-income Americans who face a marginal tax rate of 10 percent or less, and lack the ability to place the maximum allowed amount in their savings accounts.
A deeper disadvantage is that such accounts tend to undermine employment-based health care, because they encourage adverse selection: health savings accounts are attractive to healthier individuals, who will be tempted to opt out of company plans, leaving less healthy individuals behind.
Yet another problem with consumer-directed care is that the evidence says that people don’t, in fact, make wise decisions when paying for medical care out of pocket. A classic study by the Rand Corporation found that when people pay medical expenses themselves rather than relying on insurance, they do cut back on their consumption of health care—but that they cut back on valuable as well as questionable medical procedures, showing no ability to set sensible priorities.
It’s worse than, that, though.
But perhaps the biggest objection to consumer-directe health reform is that its advocates have misdiagnosed th problem. They believe that Americans have too muc health insurance; the 2004 Economic Report of the President condemned the fact that insurance currently pays for “many events that have little uncertainty, such as routine dental care, annual medical exams, and vaccinations,” and for “relatively low-expense items, such as an office visit to the doctor for a sore throat.” The implication is that health costs are too high because people who don’t pay their own medical bills consume too much routine dental care and are too ready to visit the doctor about a sore throat. And that argument is all wrong. Excessive consumption of routine care, or small-expense items, can’t be a major source of health care inefficiency, because such items don’t account for a major share of medical costs.
Remember the 80–20 rule: the great bulk of medical expenses are accounted for by a small number of people requiring very expensive treatment. When you think of the problem of health care costs, you shouldn’t envision visits to the family physician to talk about a sore throat; you should think about coronary bypass operations, dialysis, and chemotherapy. Nobody is proposing a consumer-directed health care plan that would force individuals to pay a large share of extreme medical expenses, such as the costs of chemotherapy, out of pocket. And that means that consumer-directed health care can’t promote savings on the treatments that account for most of what we spend on health care.
The administration’s plans for consumer-directed health care, then, are a diversion from meaningful health care reform, and will actually worsen our health care problems. In fact, some reformers privately hope that George W. Bush manages to get his health care plans passed, because they believe that they will hasten the collapse of employment-based coverage and pave the way for real reform. (The suffering along the way would be huge.)
The obvious answer, of course, is universal single-payer health care. I won’t try to summarize the case here (read the whole thing), but the real problem is political, not medical or economic.
We believe that the compromise plans being proposed by the cautious reformers would run into the same political problems, and that it would be politically smarter as well as economically superior to go for broke: to propose a straightforward single-payer system, and try to sell voters on the huge advantages such a sys-tem would bring. But this would mean taking on the drug and insur-ance companies rather than trying to co-opt them, and even progressive policy wonks, let alone Democratic politicians, still seem too timid to do that.
So what will really happen to American health care? Many people in this field believe that in the end America will end up with national health insurance, and perhaps with a lot of direct government provision of health care, simply because nothing else works. But things may have to get much worse before reality can break through the combination of powerful interest groups and free-market ideology.